Conscious processing of global and local auditory irregularities causes differentiated heartbeat-evoked responses
- Laboratoire de Neurosciences Cognitives et Computationnelles, Département d’Etudes Cognitives, École Normale Supérieure, INSERM, Université PSL, France
- Sorbonne Université, Paris Brain Institute (ICM), INRIA, CNRS, INSERM, AP-HP, Hôpital Pitié-Salpêtrière, France
- Institute of Neuroscience and Medicine (INM-7: Brain and Behaviour), Forschungszentrum Jülich, Germany
- Institute of Systems Neuroscience, Heinrich Heine University Düsseldorf, Germany
- AP-HP, Hôpital de la Pitié Salpêtrière, Neuro ICU, DMU Neurosciences, France
- Pitié-Salpêtrière Faculty of Medicine, Pierre and Marie Curie University, Sorbonne Universities, France
- INSERM, National Institute of Health and Medical Research, France
- Department of Neurology, Pitié-Salpêtrière Hospital Group, Public Hospital Network of Paris, France
- Department of Neurophysiology, Pitié-Salpêtrière Hospital Group, Public Hospital Network of Paris, France
Abstract
Recent research suggests that brain-heart interactions are associated with perceptual and self-consciousness. In this line, the neural responses to visceral inputs have been hypothesized to play a leading role in shaping our subjective experience. This study aims to investigate whether the contextual processing of auditory irregularities modulates both direct neuronal responses to the auditory stimuli (ERPs) and the neural responses to heartbeats, as measured with heartbeat-evoked responses (HERs). HERs were computed in patients with disorders of consciousness, diagnosed with a minimally conscious state or unresponsive wakefulness syndrome. We tested whether HERs reflect conscious auditory perception, which can potentially provide additional information for the consciousness diagnosis. EEG recordings were taken during the local-global paradigm, which evaluates the capacity of a patient to detect the appearance of auditory irregularities at local (short-term) and global (long-term) levels. The results show that local and global effects produce distinct ERPs and HERs, which can help distinguish between the minimally conscious state and unresponsive wakefulness syndrome patients. Furthermore, we found that ERP and HER responses were not correlated suggesting that independent neuronal mechanisms are behind them. These findings suggest that HER modulations in response to auditory irregularities, especially local irregularities, may be used as a novel neural marker of consciousness and may aid in the bedside diagnosis of disorders of consciousness with a more cost-effective option than neuroimaging methods.
Editor's evaluation
This study shows that neural responses to sounds and to heartbeats are affected in different ways by short-term and long-term auditory irregularities in patients diagnosed with a minimally conscious state or unresponsive wakefulness syndrome. While the findings would have been more robust had the authors collected data in the same way from a larger group of control subjects, they highlight the potential value of using heartbeat-evoked responses to inform the bedside diagnosis of disorders of consciousness. More generally, they will of interest to researchers studying brain-body interactions and their relationship to perceptual awareness.
https://doi.org/10.7554/eLife.75352.sa0Introduction
Theoretical developments in consciousness and experimental research have rooted the basis of consciousness in how the brain responds to visceral inputs (Azzalini et al., 2019; Candia-Rivera, 2022a; Park and Tallon-Baudry, 2014). In post-comatose patients, the consciousness diagnosis is primarily based on behavioral signs of consciousness (Bayne et al., 2017), which aims at distinguishing between patients showing only reflex-like responses to the environment, diagnosed as Vegetative State or Unresponsive Wakefulness Syndrome (VS/UWS; Laureys et al., 2010), and patients with fluctuating but reproducible signs of non-reflex behavior, diagnosed as a Minimally Conscious State (MCS), (Giacino et al., 2002), but see also Naccache, 2018. However, recent results demonstrate that behavioral assessment is not sufficient and neuroimaging techniques are used to detect covert states of consciousness (Kondziella et al., 2020).
The classification of MCS and UWS patients using EEG and cardiac features while undergoing processing of auditory regularities has shown an advantage over EEG features alone (Raimondo et al., 2017), implying that brain-heart interactions may be involved in the conscious processing of auditory inputs. Recent evidence on automatic classifications of HERs in the resting-state showed that these markers may capture residual signs of consciousness (Candia-Rivera et al., 2021a; Candia-Rivera and Machado, 2023a) suggesting that HERs might convey state-of-consciousness relevant information about how the brain responds to bodily-related stimuli. Further evidence exists in healthy participants, in which the processing of auditory stimuli may cause cognitive modulations to the cardiac cycle (Tanaka et al., 2023; Marshall et al., 2022; Banellis and Cruse, 2020; Perez et al., 2020; Pfeiffer and De Lucia, 2017), and HERs correlate with perceptual awareness (Al et al., 2020; Banellis and Cruse, 2020; Park et al., 2014).
We hypothesized that HERs can be modulated by contextual processing of different levels of auditory regularities, as presented in the local-global paradigm (Bekinschtein et al., 2009). In this study, we analyze HERs following the presentation of auditory irregularities, with special regard for distinguishing UWS (n=40) and MCS (n=46) patients. Note that the automated classification of this cohort was previously performed in another study (Raimondo et al., 2017). Therefore, our aim is to characterize the group-wise differences between UWS and MCS patients that may allow a multi-dimensional cognitive evaluation to infer the presence of consciousness (Sergent et al., 2017), but also complement the bedside diagnosis performed with neuroimaging methods that capture neural correlates of covert consciousness (Sanz et al., 2021).
Results
This study employed high-density EEG recordings to assess the cognitive processing of auditory irregularities in patients with disorders of consciousness using the local-global paradigm (Bekinschtein et al., 2009). This paradigm evaluates auditory regularities at both short-term (local) and long-term (global) levels within trials of five consecutive sounds. The 5th sound distinguishes standard from deviant trials at both local and global levels. As depicted in Figure 1A, XX, and XY types of blocks were presented. In XX blocks, frequent stimuli consisted of five equal sounds (local and global standard), whereas infrequent stimuli had four equal sounds followed by a different 5th sound (local and global deviant). In XY blocks, frequent stimuli involved four equal sounds followed by a different 5th sound (local deviant and global standard), while infrequent stimuli featured five equal sounds (local standard and global deviant). We examined the cognitive processing of auditory irregularities with the objective to identify the physiological responses that could differentiate between patients in MCS and those in UWS. We hypothesized that assessing auditory irregularities at both local and global levels could offer valuable insights into the distinction of MCS and UWS patients. Furthermore, that distinction may be further improved by analyzing the physiological modulation of auditory processing in relation to measures of brain-heart interactions. To achieve this, we conducted tests to investigate the local and global effects of ERPs, which involved analyzing the standard average of EEG epochs aligned with the occurrence of auditory deviants (Figure 1B). Additionally, we explored the HERs, which involved analyzing the average of EEG epochs aligned with the occurrence of heartbeats following the auditory deviants (Figure 1B). We aimed to assess whether the neural responses to heartbeats, within the context of auditory irregularity processing, could serve as novel differentiating factors between MCS and UWS patients.
Figure 1
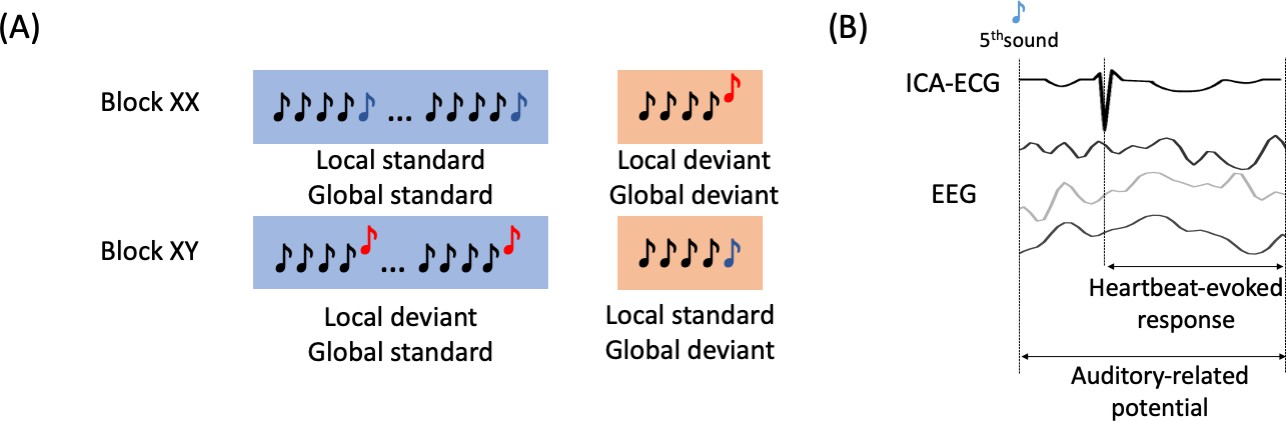
Experimental description and EEG analysis.
(A) Local-global paradigm. (B) Heartbeat-evoked response defined by the R-peaks that follow the 5th sound from all the trials, and the Auditory-related potential defined by the EEG activity locked to the stimuli.
First, unpaired non-parametric cluster analysis was performed between MCS and UWS patients for ERPs, global and local effects. The local effect involved calculating the average of EEG epochs associated with local deviants (comprising local deviant/global standard epochs and local deviant/global deviant epochs) and subtracting the average of the EEG epochs associated with local standards (comprising local standard/global standard epochs and local standard/global deviant epochs). The global effect involved calculating the average of EEG epochs linked to global deviants (comprising local standard/global deviant epochs and local deviant/global deviant epochs) and subtracting the average of EEG epochs associated with global standards (comprising local standard/global standard epochs and local deviant/global standard epochs). Figure 2A shows the clustered effects found with respect to the 5th sound, in the ERP global effect (main positive cluster: p=0.0001, Z=3.684, latency = 800–850 ms; main negative cluster: p=0.0013, Z=–3.1905, latency = 280–336 ms) and ERP local effect (main positive cluster: p=0.0011, Z=3.4416, latency = 236–328 ms). The clustered effects were combined to obtain a single value for each patient, corresponding to ERP global and local effects. To combine the clustered effects, we computed the average of all points (channel × time) identified in the cluster permutation analysis, which effectively distinguished between patients diagnosed with MCS and UWS. The distribution of the combined clustered effects are depicted in Figure 2B and the time course of one of the channels of the cluster in Figure 2C.
Figure 2
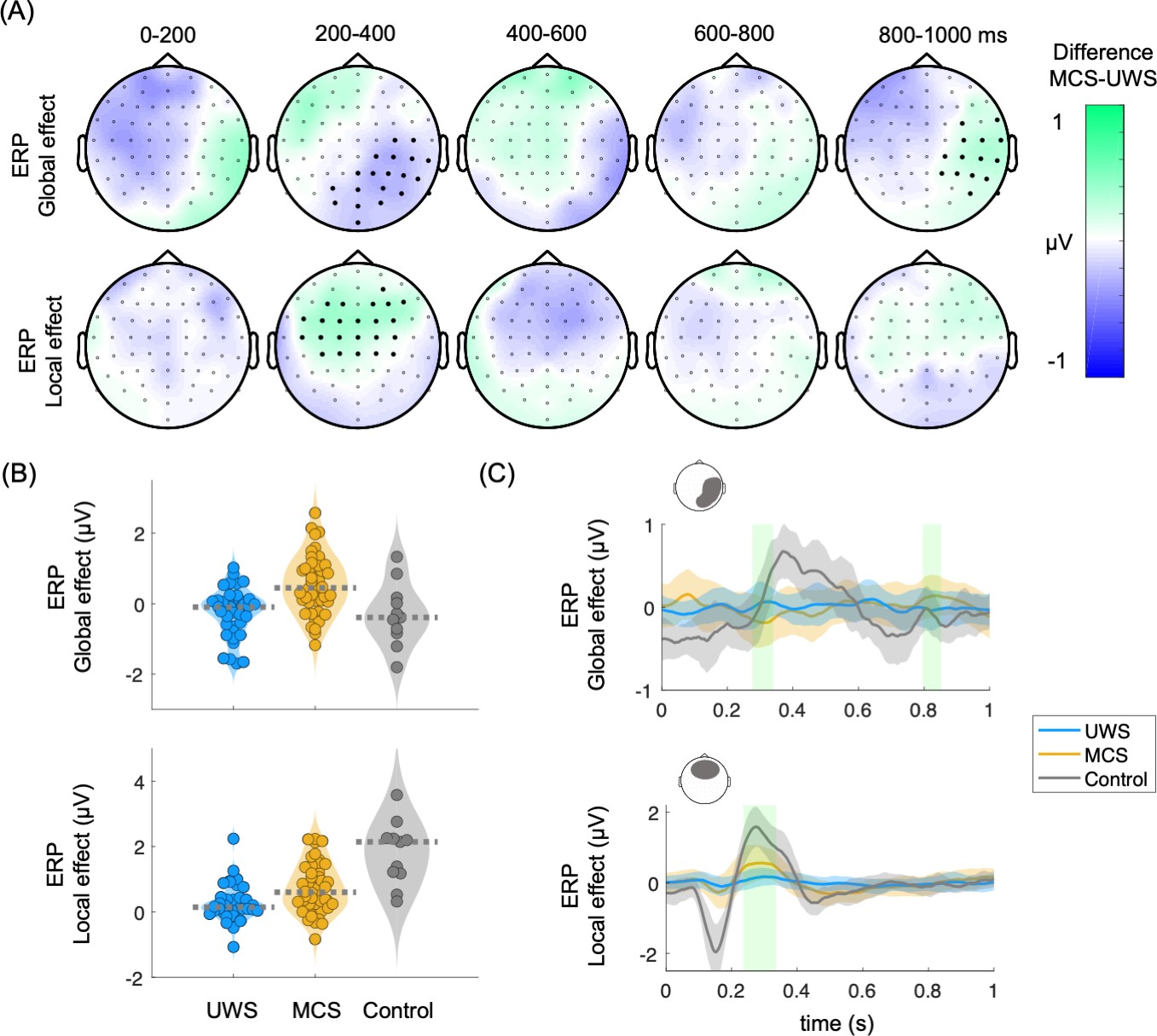
Auditory event-related potentials (ERPs) in the global and local effects.
(A) Scalp topographies indicate the average group differences between MCS and UWS patients. Thick electrodes indicate a clustered effect (Monte Carlo p<0.05). (B) Average of the clustered effects per patient, in the ERP global effect (main positive cluster: p=0.0001, Z=3.684, latency = 800–850 ms; main negative cluster: p=0.0013, Z=–3.1905, latency = 280–336 ms), and ERP local effect (main positive cluster: p=0.0011, Z=3.4416, latency = 236–328 ms). Healthy controls are displayed as a reference. Dashed lines indicate the group median (C) Time course of the group median among UWS, MCS, and control groups. The displayed time course corresponds to the scalp area marked above the corresponding plot. Shaded green areas indicate the segments in which a clustered effect was found when comparing MCS and UWS groups. ERPs: auditory event-related potentials, MCS: minimally conscious state, UWS: unresponsive wakefulness syndrome.
Consecutively, cluster permutation analysis was performed between MCS and UWS patients for HERs, global and local effects. In Figure 3A are shown the clustered effects found with respect to the R-peak following the 5th sound, in the HER global effect (main positive cluster: p=0.0037, Z=3.0173, latency = 112–130 ms; main negative cluster: p0.0058, Z=–3.0173, latency = 340–360 ms) and HER local effect (main positive cluster: p=0.0029, Z=3.0606, latency = 400–412 ms; main negative cluster: p=0.0014, Z=–3.3983, latency = 0–40 ms). The clustered effects were combined to obtain a single value for each patient, corresponding to HER global and local effects. The distribution of the combined clustered effects are depicted in Figure 3B and the time course of one of the channels of the cluster in Figure 3C. The combined clustered effects were compared to 100 randomly distributed heartbeats to compute the surrogate p-value. The HER local effect was larger than what would be expected by chance as estimated from surrogate heartbeats (HER local effect, Monte Carlo p=0.03; HER global effect, Monte Carlo p=0.54).
Figure 3
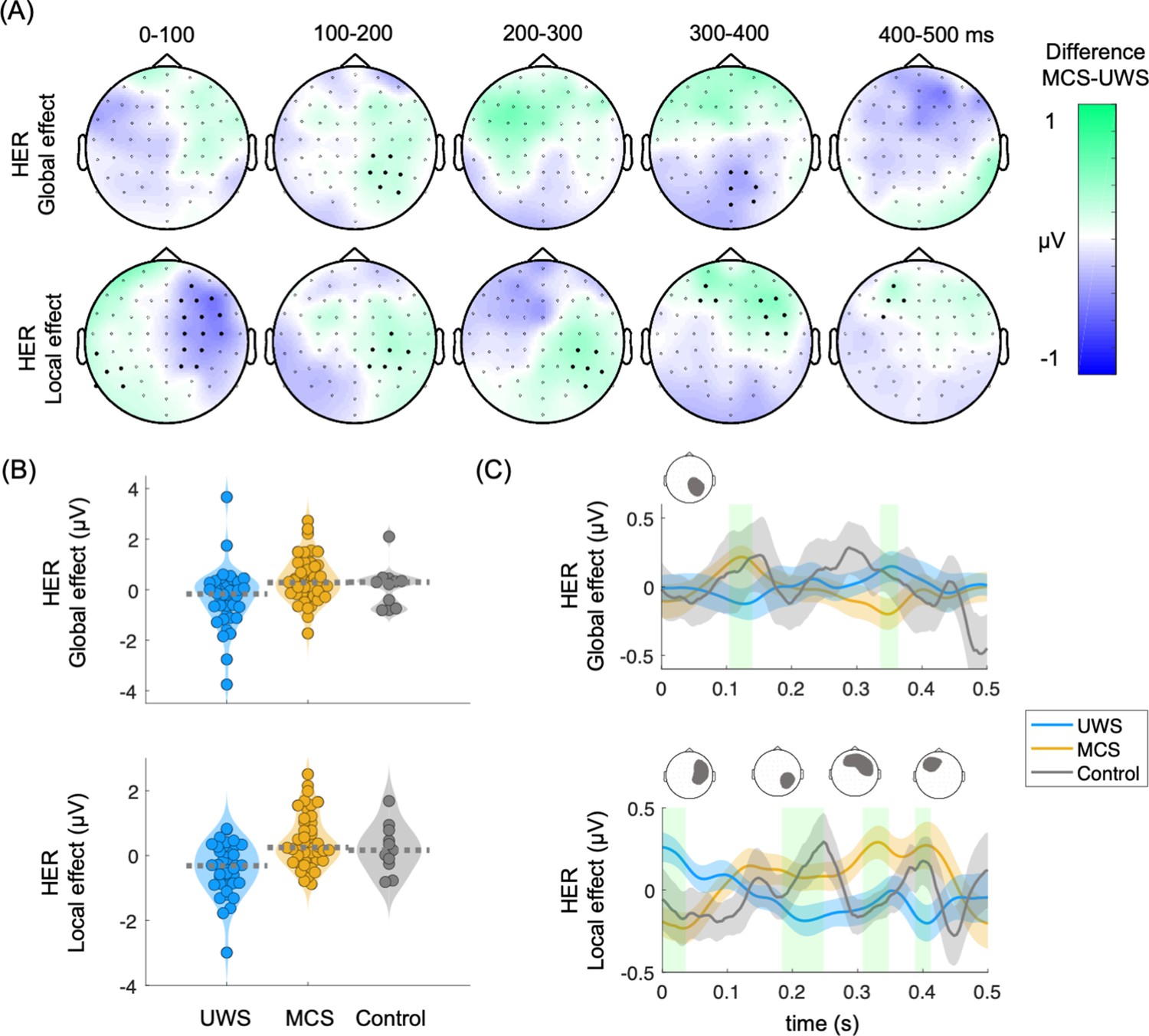
Heartbeat-evoked responses (HERs) in the global and local effects.
(A) Scalp topographies indicate the average group differences between MCS and UWS patients. Thick electrodes indicate a clustered effect (Monte Carlo p<0.05). (B) Average of the clustered effects per patient, in the HER global effect (main positive cluster: p=0.0037, Z=3.0173, latency = 112–130 ms; main negative cluster: p=0.0058, Z=–3.0173, latency = 340–360 ms) and HER local effect (main positive cluster: p=0.0029, Z=3.0606, latency = 400–412 ms; main negative cluster: p=0.0014, Z=–3.3983, latency = 0–40 ms). Healthy controls are displayed as a reference. Dashed lines indicate the group median (C) Time course of the group median among UWS, MCS, and control groups. The displayed time course corresponds to the scalp area marked above the corresponding plot. Shaded green areas indicate the segments in which a clustered effect was found when comparing MCS and UWS groups. HERs: heartbeat-evoked responses, MCS: minimally conscious state, UWS: unresponsive wakefulness syndrome.
We then tested whether the clusters found using cluster permutations at global and local effects, as measured from HERs and ERPs, come from a distribution with a median different from zero, i.e., whether the deviants differ from the standard 5th sounds within patients' groups (Table 1). We found a significant ERP and HER local effect in both MCS and UWS patients. On the other hand, the global effect was significant only for MCS patients in both ERP and HER analysis. This result extends previous reports highlighting the predictive power for the conscious state of the global effect (Pérez et al., 2021).
Table 1
Wilcoxon sign test performed separately for MCS and UWS patients, to test whether the global and local effects as measured from HERs and ERPs come from a distribution with median different to zero.
Bold indicates significance reached at α=0.05/8=0.0063, according to Bonferroni correction for multiple comparisons.
| Patients | HERs | ERPs | ||
|---|---|---|---|---|
| Global effect | Local effect | Global effect | Local effect | |
| MCS | Z=2.7805 p=0.0054 | Z=3.2175 p=0.0013 | Z=3.7529 p=0.0002 | Z=5.0311 p<0.0001 |
| UWS | Z=–1.9759 p=0.0482 | Z=–2.9840 p=0.0028 | Z=–1.9624 p=0.0497 | Z=2.9033 p=0.0037 |
-
HERs: heartbeat-evoked responses, ERPs: auditory event-related potentials, MCS: minimally conscious state, UWS: unresponsive wakefulness syndrome.
In Figure 4A are presented all pair comparisons between ERPs and HERs. for local and global effects. The figure depicts that the measured effects do not show apparent correlations (details on Spearman correlation tests in Table 2). Figure 4B shows that the four markers: ERP global, ERP local, HER global, and HER local present complementary information for the separation of the diagnostic groups.
Figure 4
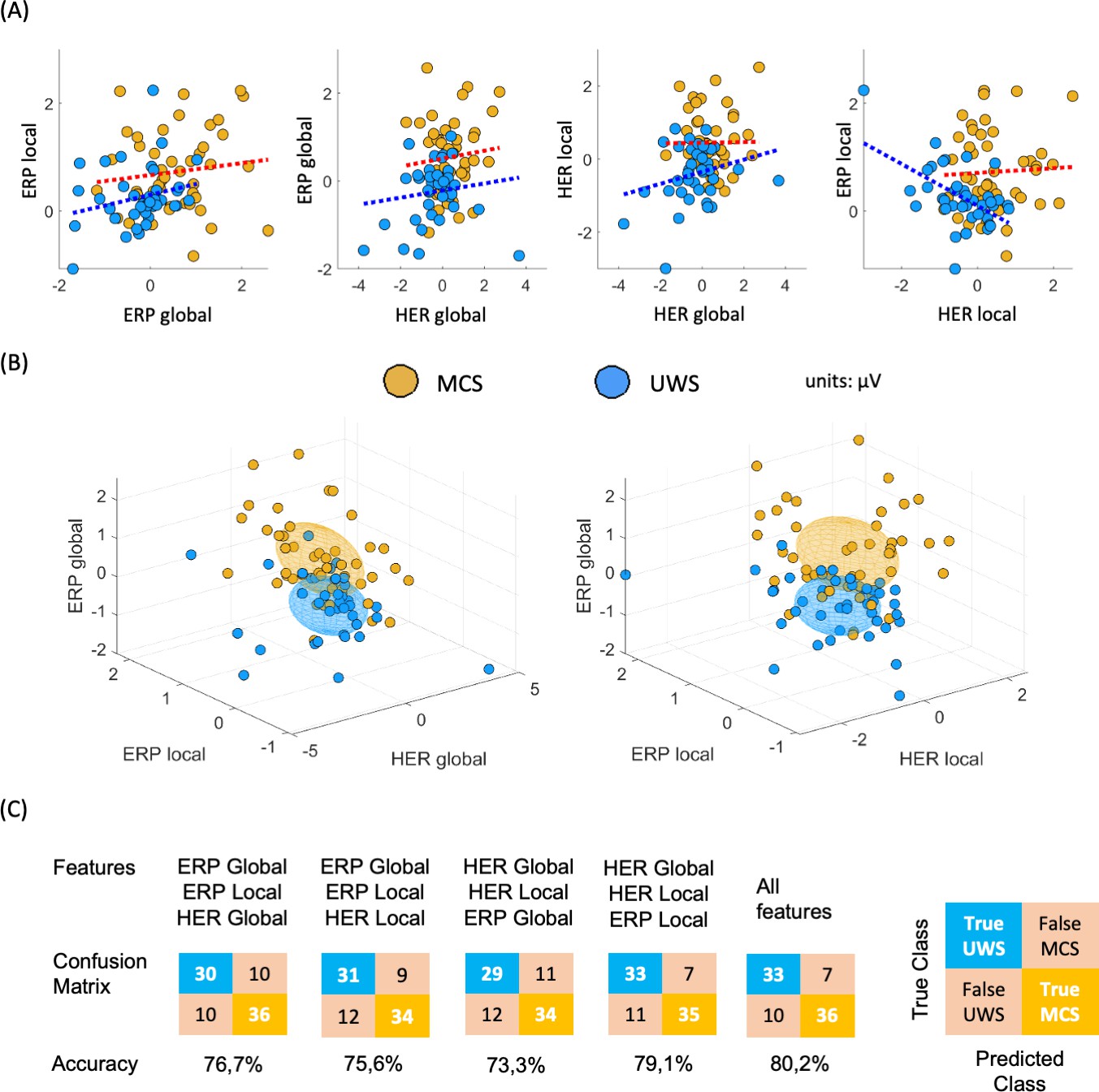
Multi-dimensional analysis of the clustered effects found when comparing MCS and UWS patients.
(A) Pairwise comparison between all possible combinations for ERPs and HERs, for local and global effects. Individual points corresponding to a single patient, and dotted line indicates the trend, separately per diagnosis. (B) Three-dimensional representation of the clustered effects: left panel for ERP global, ERP local, and HER global; and right panel for ERP global, ERP local, and HER local. Each ellipsoid was constructed per diagnostic group, centered in the group means with a ratio defined by the standard deviations, for the respective dimensions. (C) Confusion matrices depicting the classification results of MCS and UWS patients using a linear discriminant classifier in a fivefold cross-validation. The classifiers were trained using all possible combinations of feature triads, as well as all four features. HERs: heartbeat-evoked responses, ERPs: auditory event-related potentials, MCS: minimally conscious state, UWS: unresponsive wakefulness syndrome.
Table 2
Group-wise Spearman correlation analysis performed separately for MCS and UWS patients, between the combined clustered effects found when comparing MCS vs UWS in the ERP global effect, ERP local effect, HER global effect, and HER local effect.
Significance was set at α=0.05/8=0.0063, according to Bonferroni correction for multiple comparisons.
| MCS | UWS | |
|---|---|---|
| ERP global vs ERP local | R=0.1077 p=0.4748 | R=0.3099 p=0.0591 |
| HER global vs ERP global | R=0.0575 p=0.7033 | R=0.1580 p=0.3290 |
| HER global vs HER local | R=–0.1193 p=0.4283 | R=0.1480 p=0.3607 |
| HER local vs ERP local | R=–0.0436 p=0.7730 | R=–0.4114 p=0.0088 |
-
HER: heartbeat-evoked response, ERP: auditory event-related potential, MCS: minimally conscious state, UWS: unresponsive wakefulness syndrome.
To further demonstrate the discrimination power of MCS and UWS patients using HERs and ERPs, we employed a linear discriminant classifier in a fivefold cross-validation. Figure 4C illustrates that combining HER local, ERP global, and ERP local offered the most complementary information out of all possible triads, achieving a cross-validation accuracy of 79.1%. The accuracy further improved to 80.2% when incorporating the four features. These findings highlight the additional insights provided by HERs in conjunction with the standard ERP analysis.
HER average during the whole protocol presents a small, clustered effect when comparing MCS and UWS patients (Figure 5A, left). In Figure 5A, the right panel is shown that a higher HER variance is observed in MCS compared to UWS during the whole protocol. A wide scalp coverage presents higher HER variance in MCS, as compared to UWS (cluster permutation test, p<0.0001, Z=4.0772, latency = 20–500 ms). The time courses of the clustered effects in HER average and variance are shown in Figure 5B.
Figure 5
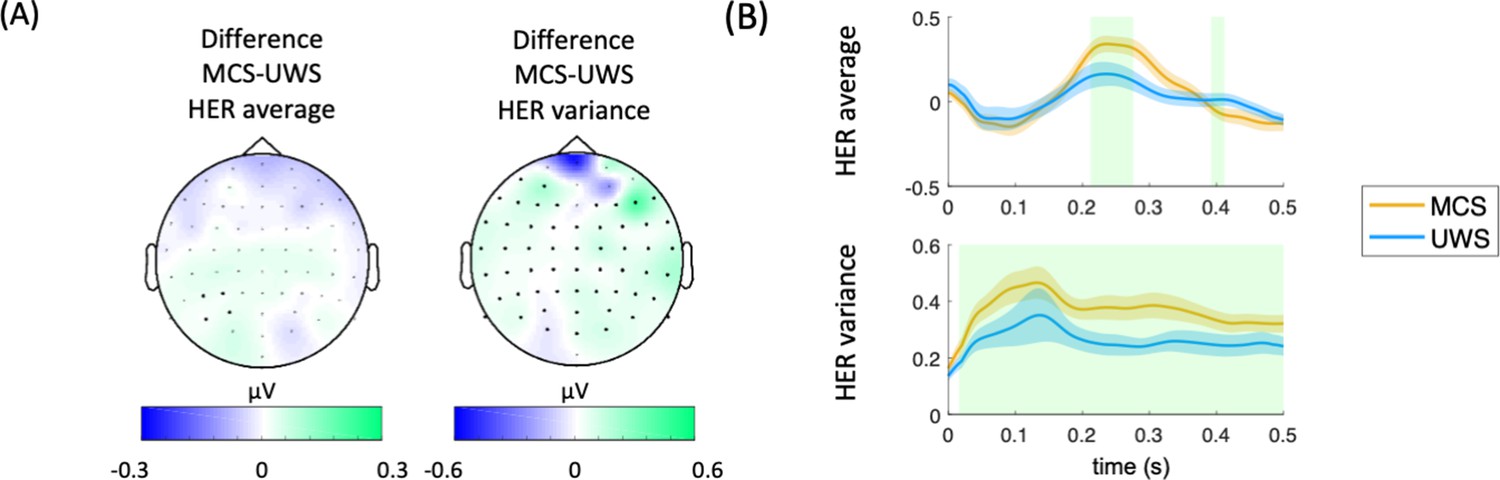
Results on HER average and HER variance for the whole protocol.
(A) HER scalp topographies of the differences between MCS and UWS patients. Thick electrodes show significant differences after cluster permutation. (B) HER variance in MCS and UWS patients in the significant cluster. Shaded green areas indicate the segments in which a clustered effect was found when comparing MCS and UWS groups. HERs: heartbeat-evoked responses, MCS: minimally conscious state, UWS: unresponsive wakefulness syndrome.
Discussion
Considering that brain-heart interactions have demonstrated to be involved in consciousness and relevant for the clinical assessment of brain-injured patients (Candia-Rivera et al., 2021a; Candia-Rivera and Machado, 2023b; Perez et al., 2020; Raimondo et al., 2017; Riganello et al., 2019), we analyzed neural responses to heartbeats during the processing of auditory irregularities to characterize MCS and UWS patients. The processing of short- and long-term auditory irregularities, i.e., the local and global effects, shows distinctive responses between MCS and UWS patients in their HERs.
The correlation analyses revealed that the EEG signals synchronized to heartbeats (HERs) provided complementary information to the ERPs synchronized to auditory irregularities. Examining the local effects using HERs and ERPs yielded better differentiability between MCS and UWS patients (see Figure 5).
It is worth noting that the HER local effect demonstrated higher specificity, as compared to the HER global effect during the permutation test. Only 3% of randomly timed surrogate heartbeats exhibited separability that surpassed what was observed with the original heartbeats. These results align with previous findings that suggest the existence of a short-term auditory-cardiac synchrony (Banellis and Cruse, 2020; Pérez et al., 2021; Pfeiffer and De Lucia, 2017). Moreover, our findings indicate that brain-heart dynamics may serve as markers of the conscious processing of auditory information, particularly in distinguishing short-term changes.
Our results go in the same direction as previous evidence, in which automatic classifications of these patients showed a higher accuracy when locking EEG to heartbeats, with respect to the classification of EEG segments unrelated to the cardiac cycle (Candia-Rivera et al., 2021a). Nevertheless, the measured responses in ERPs and HERs do not separate MCS and UWS patients’ groups completely (see Figure 4C), suggesting that some patients do not react or only react to some trials that were attenuated when averaging all trials in the time-locked analysis. Furthermore, it is worth noting that the ERP global effect observed in healthy controls did not follow the same trend as MCS patients. These findings may require of further future explorations to determine if the observed effect is exclusive to MCS patients or if healthy controls do not exhibit the same effect due to their lower number of trials performed in the local-global paradigm during this study. However, the response observed in healthy controls does resemble a standard P300 response. These findings align with previous reports indicating that the ERPs during local deviants exhibit superior discriminatory ability between MCS and UWS patients (Faugeras et al., 2012). Furthermore, these results suggest that both ERP and HER in processing local auditory irregularities might be predominant for distinguishing between MCS and UWS. This notion is further supported by the higher accuracy of the linear discriminant classifier in classifying MCS and UWS patients by using ERP local and both HER global and local effects, as compared to all other possible feature combinations. Nonetheless, the inclusion of global effects marginally improved the classification performance, indicating that although the global effects are weaker than the local effects, they might provide complementary information to the local effects.
Our results contribute to the extensive experimental evidence showing that brain-heart interactions, as measured with HERs, are related to perceptual awareness (Azzalini et al., 2019; Skora et al., 2022). For instance, neural responses to heartbeats correlate with perception in a visual detection task (Park et al., 2014). Further evidence exists on somatosensory perception, where a higher detection of somatosensory stimuli occurs when the cardiac cycle is in diastole and it is reflected in HERs (Al et al., 2020). Evidence on heart transplanted patients show that the ability of heartbeats sensation is reduced after surgery and recovered after one year, with the evolution of the heartbeats sensation recovery reflected in the neural responses to heartbeats as well (Salamone et al., 2020). The responses to heartbeats also covary with self-perception: bodily-self-identification of the full body (Park et al., 2016), and face (Sel et al., 2017), and the self-relatedness of spontaneous thoughts (Babo-Rebelo et al., 2016) and imagination (Babo-Rebelo et al., 2019). Moreover, brain-heart interactions measured from heart rate variability correlate with conscious auditory perception as well (Banellis and Cruse, 2020; Pérez et al., 2021; Pfeiffer and De Lucia, 2017).
We showed that ERPs and HERs are repeatedly larger in MCS patients, as compared to UWS, in both local and global effects. Furthermore, the ERPs and HERs (both for the local and global effects) are uncorrelated in all possible comparisons (see Figure 4A), in addition to the results show differentiation of clustering effects in HER and ERP (see Figure 4B). These results suggest that the neuronal mechanisms behind these ERPs and HERs responses are independent. In addition, we found that HER variance is higher in MCS patients than in UWS patients, as previously reported in resting state (Candia-Rivera and Machado, 2023a). These results suggest that there are two distinct neuronal signatures that set apart patients in a MCS from those in an UWS. A first process probed with HER variability differentiates, irrespective of the current stimulus types being processed. This first process originates from the central and right temporal scalp areas and has been linked with social cognition but could also correspond to a self-consciousness-state markers (Candia-Rivera et al., 2021a). Second, a modulation of HER in response to local and global auditory irregularities. These responses present several properties related to a neural signature of conscious access to local and global deviant stimuli. Such ERPs and HERs modulations by conscious access to a new stimulus attribute may well correspond to a self-consciousness updating process occurring ‘downstream’ to conscious access (Sergent and Naccache, 2012), and enabled, for instance, in a global neuronal workspace architecture (Dehaene and Naccache, 2001).
Note that outliers are expected in disorders of consciousness, and an exact physiological characterization of the different levels of consciousness remains challenging. First, the standard assessment of consciousness based on behavioral measures has shown a high rate of misdiagnosis in MCS and UWS (Stender et al., 2014). The cause of the misdiagnosis of consciousness arises because consciousness does not necessarily translate into overt behavior (Hermann et al., 2021). Unresponsive and minimally conscious patients, namely non-behavioral MCS (Thibaut et al., 2021), represents the main diagnostic challenge in clinical practice. Second, some of these patients suffer from conditions that may translate into no response to stimuli, even in the presence of consciousness. For instance, when they suffer from constant pain, fluctuations in arousal levels, or sensory impairments caused by brain damage (Chennu et al., 2013). Third, these patients were recorded in clinical setups, which may lead to a lower signal-to-noise ratio, and consecutively lead to biased measurements in evoked potentials (Clayson et al., 2013).
A plethora of complementary neuroimaging techniques have been proposed to enhance the consciousness diagnosis, including anatomical and functional magnetic resonance imaging and positron emission tomography (Kondziella et al., 2020; Sanz et al., 2021). However, those methodologies may not be accessible in all clinical setups, because of costs or medical contraindications. The foregoing evidence of EEG-based techniques to diagnose consciousness (Bai et al., 2021; Engemann et al., 2018) shows promising and low-cost opportunities to develop diagnostic methods that can capture residual consciousness. Our results contribute more evidence of the potential of EEG as a diagnostic tool, but also to the role of visceral signals in consciousness (Azzalini et al., 2019; Candia-Rivera, 2022a; Sattin et al., 2020). This study gives evidence that HERs detect auditory conscious perception, in addition to the residual signs of consciousness in the resting-state (Candia-Rivera et al., 2021a).
Materials and methods
Patients
This study includes 46 MCS, 40 UWS patients, and 11 healthy controls. Patients were admitted at the Department of Neurology, Pitié-Salpêtrière Hospital (Paris, France) for consciousness evaluation through Coma Recovery Scale-Revised (CRS-R) (Giacino et al., 2004).
The study was approved by the local ethics committee (Ethical committee of the French Society of Intensive Care Medicine - SRLF; Paris, France, NEURO-DoC/HAO-006/20130409, and M-NEURO-DoC/NCT04534777). Informed consent was signed by the patients’ legal representatives for approval of participation in the study, as required by the declaration of Helsinki.
Experimental paradigm
Request a detailed protocolPatients were recorded with high-density EEG (EGI 256 channels, 250 Hz sampling rate, referenced to the vertex) under the local-global paradigm that aims to evaluate the cognitive processing of local–short-term–, and global–long-term–auditory regularities (Figure 1A; Bekinschtein et al., 2009). The paradigm consists of two embedded levels of auditory regularities in trials formed by five consecutive sounds. The 5th sound defines whether the trial is standard or deviant at two levels: local and global. The local level of regularity is defined within the trial. The global level of regularities is defined across trials (frequent trials ~80% define the regularity, and rare ones ~20% violate this regularity). In Figure 1A, in the XX blocks, the frequent stimulus corresponds to five equal sounds (local standard and global standard). In contrast, the infrequent stimulus corresponds to four equal sounds followed by a fifth different sound (local deviant and global deviant). In the XY blocks, the frequent stimulus corresponds to four equal sounds and a fifth different sound (local deviant and global standard). The infrequent stimulus corresponds to five equal sounds (local standard and global deviant). The patients included in this study performed at least four blocks (2 XX and 2 XY), in which one block has an approximate duration of 200 s. Each trial is formed by five consecutive sounds lasting 50 milliseconds, with a 150 millisecond gap between the sounds’ onsets and an intertrial interval ranging from 1350–1650 milliseconds.
The healthy controls participating in this study completed two blocks of the local-global paradigm, one XX and one XY. It is important to note that they were included solely as a reference group for qualitative analyses. The purpose of including healthy controls in our study was to determine if MCS patients exhibit similar trends in markers where a differentiation between MCS and UWS/VS patients was observed.
Data preprocessing
Request a detailed protocolMATLAB and Fieldtrip toolbox were used for data processing and analysis (Oostenveld et al., 2011). EEG data were offline filtered with a 1–25 Hz Butterworth band-pass order four filter, with a Hamming windowing at cutoff frequencies. The channels with large artifacts were rejected based on the area under the curve of their z-score. Channels exceeding >3 standard deviations were discarded iteratively (11±1 SEM channels rejected on average). Following the procedure described in Raimondo et al., 2017, electrocardiograms (ECG) were recovered from the cardiac field artifact captured in EEG data using Independent Component Analysis (ICA) (default parameters from Fieldtrip). From this, ICA-corrected EEG data and an electrocardiogram derived from independent component analysis (ICA-ECG) is obtained. Note that the use of ICA-ECG instead of a standard ECG measured from the rib cage was successfully used in other two studies (Candia-Rivera et al., 2021a; Raimondo et al., 2017). Furthermore, it was shown that the differences between the R-peak timings obtained from the ECG and ICA-ECG differ in a range of 0–4 ms (Candia-Rivera et al., 2021a).
To identify further noisy channels, the mean weighted-by-distance correlation of all channels between their neighbors were computed (36±2 SEM channels rejected on average). Neighborhood relationships considered all channels up to distances of 4 cm. Channels with a mean weighted-by-distance correlation lower than 80% were replaced by spline interpolation of neighbors. EEG dataset was re-referenced using a common average and a subset of 64 channels were selected for data analysis (Candia-Rivera et al., 2021b).
Heartbeats were detected on the ICA-ECG using an automated process based on a sliding time window detecting local maxima (R-peaks). Both peak detection and resulting histograms of interbeat interval duration were visually inspected in each patient. Ectopic interbeat intervals were automatically identified for review by detecting peaks on the derivative of the interbeat intervals time series. Manual addition/removal of peaks was performed if needed (23±3 SEM manual corrections to individual heartbeats on average).
HERs (Park and Blanke, 2019; Schandry et al., 1986) were computed by averaging EEG epochs from the R-peaks that follow the 5th sound from all the trials, up to 500 ms (Figure 1B). Epochs with amplitude larger than 300 μV on any channel, or where the next or preceding heartbeat occurred at an interval shorter than 500 ms, were discarded. The epochs in which the stimuli were located at less than 20 ms from the closest R-peaks were discarded as well. We also controlled that the average latency between the 5th sound and the next heartbeat did not differ between MCS and UWS patients (Wilcoxon tests, local standard: p=0.2303, Z=1.1991; local deviants: p=0.3387, Z=0.9567; global standard: p=0.2047, Z=1.2684; global deviant: p=0.4182, Z=0.8095).
Auditory event-related potentials (ERPs) were computed for contrast by averaging EEG epochs from the 5th sound onset from all the trials, up to 1000 ms. Epochs with amplitude larger than 300 μV on any channel were discarded.
Data analysis
Request a detailed protocolTwo neural signatures were computed to compare MCS and UWS patients: ERPs, that relate to the average of EEG epochs locked to the auditory stimuli, and HERs that relate to the average of EEG epochs locked to the heartbeats that follow the auditory stimuli. The experimental conditions, in which ERPs and HERs were used to compare MCS and UWS patients, are:
Local effect: average of the EEG epoch associated with local deviants (local deviant/global standard epochs + local deviant/global deviant epochs), minus the average of EEG epochs associated with local standards (local standard/global standard epochs + local standard/global deviant epochs).
Global effect: average of the EEG epoch associated to global deviants (local standard/global deviant epochs + local deviant/global deviant epochs), minus the average of EEG epochs associated to global standards (local standard/global standard epochs + local deviant/global standard epochs).
Additionally, HERs average and HERs variance were analyzed during the whole experimental protocol, i.e., the neural responses to heartbeats were analyzed with respect to all heartbeats independently of stimuli.
Statistical analysis
Request a detailed protocolStatistical comparisons were based on Wilcoxon rank sum and Spearman correlation, as specified in the main text. p-values were corrected for multiple comparisons by applying the Bonferroni rule or by using cluster-permutation analyses.
Clustered effects were revealed using a non-parametric version of cluster permutation analysis (Candia-Rivera and Valenza, 2022b). In brief, the cluster-based permutation test included a preliminary mask definition, identification of candidate clusters, and the computation of cluster statistics with Monte Carlo’s p-value correction. The preliminary mask was defined through an unpaired Wilcoxon test, with alpha = 0.05. The identification of neighbor channels were based on the default Fieldtrip channels’ neighborhood definition for 64 channels. A minimum cluster size of four channels was imposed. Adjacent candidate clusters on time were wrapped if they had at least one channel in common. Cluster statistics were computed from 10,000 random partitions. The proportion of random partitions that resulted in a lower p-value than the observed one was considered as the Monte Carlo p-value, with significance at alpha = 0.05. The cluster statistic considered is the Wilcoxon’s absolute maximum Z-value obtained from all the samples of the mask.
Additionally, to confirm the presence of true effects in HERs, we compared the combined clustered effects with surrogates. We reallocated each heartbeat timing using a uniformly distributed pseudorandom process, between the first and the last sample of each recording. We computed 100 surrogates and repeated the aforementioned statistical analysis. We computed Monte Carlo p-values as the proportion of the combined clustered effects found in the surrogates with a higher effect and cluster size, with respect to the real heartbeat timings.
Lastly, in order to assess the complementarity of clusters identified in ERPs and HERs across local and global effects, we employed a fivefold cross-validation to train a linear discriminant classifier (Fisher, 1936), as implemented in MATLAB. The accuracies and confusion matrices were reported to evaluate the performance of the features’ combinations and to quantify the occurrence of ‘false MCS’ and ‘false UWS’ predictions.
Data availability
The data used in this study can be made available upon reasonable request. Because of the sensitive nature of the clinical information concerning the patients, the ethics protocol does not allow open data sharing. To access the raw data, the potential interested researcher would need to contact the corresponding authors of the study. Together they would need to ask for an authorization from the local ethics committee, CPP Île de France 1 (Paris, France). The codes and pre-processed data are available at https://github.com/diegocandiar/brain_heart_doc, (copy archived at Candia-Rivera, 2021).
References
-
Visceral signals shape Brain dynamics and cognitionTrends in Cognitive Sciences 23:488–509.https://doi.org/10.1016/j.tics.2019.03.007
-
Neural responses to Heartbeats in the Default Network encode the self in spontaneous thoughtsThe Journal of Neuroscience 36:7829–7840.https://doi.org/10.1523/JNEUROSCI.0262-16.2016
-
Managing disorders of consciousness: the role of electroencephalographyJournal of Neurology 268:4033–4065.https://doi.org/10.1007/s00415-020-10095-z
-
Skipping a Beat: Heartbeat-Evoked potentials reflect predictions during interoceptive-exteroceptive integrationCerebral Cortex Communications 1:tgaa060.https://doi.org/10.1093/texcom/tgaa060
-
Reforming the taxonomy in disorders of consciousnessAnnals of Neurology 82:866–872.https://doi.org/10.1002/ana.25088
-
SoftwareBrain_Heart_Doc, version swh:1:rev:a61c16f8934c06783e27035b09d1d46e80f40f7cSoftware Heritage.
-
Brain-heart interactions in the neurobiology of consciousnessCurrent Research in Neurobiology 3:100050.https://doi.org/10.1016/j.crneur.2022.100050
-
Multidimensional assessment of heartbeat-evoked responses in disorders of consciousnessThe European Journal of Neuroscience 58:3098–3110.https://doi.org/10.1111/ejn.16079
-
Reduced Heartbeat-Evoked responses in a Near-Death Case ReportJournal of Clinical Neurology 19(6):581-588.https://doi.org/10.3988/jcn.2022.0415
-
Dissociable endogenous and exogenous attention in disorders of consciousnessNeuroImage. Clinical 3:450–461.https://doi.org/10.1016/j.nicl.2013.10.008
-
The use of multiple measurements in taxonomic problemsAnnals of Eugenics 7:179–188.https://doi.org/10.1111/j.1469-1809.1936.tb02137.x
-
The JFK Coma Recovery Scale-Revised: measurement characteristics and diagnostic utilityArchives of Physical Medicine and Rehabilitation 85:2020–2029.https://doi.org/10.1016/j.apmr.2004.02.033
-
Importance, limits and caveats of the use of “disorders of consciousness” to theorize consciousnessNeuroscience of Consciousness 2021:iab048.https://doi.org/10.1093/nc/niab048
-
European Academy of Neurology guideline on the diagnosis of coma and other disorders of consciousnessEuropean Journal of Neurology 27:741–756.https://doi.org/10.1111/ene.14151
-
FieldTrip: Open source software for advanced analysis of MEG, EEG, and invasive electrophysiological dataComputational Intelligence and Neuroscience 2011:156869.https://doi.org/10.1155/2011/156869
-
Spontaneous fluctuations in neural responses to heartbeats predict visual detectionNature Neuroscience 17:612–618.https://doi.org/10.1038/nn.3671
-
The neural subjective frame: from bodily signals to perceptual consciousnessPhilosophical Transactions of the Royal Society of London. Series B, Biological Sciences 369:20130208.https://doi.org/10.1098/rstb.2013.0208
-
Transient modulations of neural responses to Heartbeats Covary with bodily self-consciousnessThe Journal of Neuroscience 36:8453–8460.https://doi.org/10.1523/JNEUROSCI.0311-16.2016
-
Auditory event-related “Global Effect” predicts recovery of overt consciousnessFrontiers in Neurology 11:588233.https://doi.org/10.3389/fneur.2020.588233
-
Cardio-audio synchronization drives neural surprise responseScientific Reports 7:14842.https://doi.org/10.1038/s41598-017-13861-8
-
Brain-heart interactions reveal consciousness in noncommunicating patientsAnnals of Neurology 82:578–591.https://doi.org/10.1002/ana.25045
-
Measures of CNS-Autonomic interaction and responsiveness in disorder of consciousnessFrontiers in Neuroscience 13:530.https://doi.org/10.3389/fnins.2019.00530
-
Dynamic neurocognitive changes in interoception after heart transplantBrain Communications 2:fcaa095.https://doi.org/10.1093/braincomms/fcaa095
-
Update on neuroimaging in disorders of consciousnessCurrent Opinion in Neurology 34:488–496.https://doi.org/10.1097/WCO.0000000000000951
-
From the heart to the brain: a study of heartbeat contingent scalp potentialsThe International Journal of Neuroscience 30:261–275.https://doi.org/10.3109/00207458608985677
-
Imaging neural signatures of consciousness: “what”, “when”, “where” and “how” does it workArchives Italiennes de Biologie 150:91–106.https://doi.org/10.4449/aib.v150i2.1270
-
The functional role of cardiac activity in perception and actionNeuroscience & Biobehavioral Reviews 137:104655.https://doi.org/10.1016/j.neubiorev.2022.104655
-
Preservation of Brain activity in unresponsive patients identifies MCS StarAnnals of Neurology 90:89–100.https://doi.org/10.1002/ana.26095
Decision letter
-
Andrew J KingSenior and Reviewing Editor; University of Oxford, United Kingdom
-
Marta GarridoReviewer
-
Maria ChaitReviewer; University College London, United Kingdom
Our editorial process produces two outputs: (i) public reviews designed to be posted alongside the preprint for the benefit of readers; (ii) feedback on the manuscript for the authors, including requests for revisions, shown below. We also include an acceptance summary that explains what the editors found interesting or important about the work.
Decision letter after peer review:
Thank you for submitting your article "Processing of slow-global auditory regularities causes larger neural responses to heartbeats in patients under minimal consciousness state, compared to unresponsive wakefulness syndrome" for consideration by eLife. Your article has been reviewed by 3 peer reviewers, including Maria Chait as the Reviewing Editor and Reviewer #3, and the evaluation has been overseen by Andrew King as the Senior Editor. The following individual involved in review of your submission has agreed to reveal their identity: Marta Garrido (Reviewer #2).
The reviewers have discussed their reviews with one another, and the Reviewing Editor has drafted this to help you prepare a revised submission.
Essential revisions:
We found the work potentially very interesting, however several key issues, critical for supporting the claims in this paper, were identified. We hope you can address these in a revision.
1) We were confused by the specificity of HER differences vs straightforward prediction error differences in auditory evoked responses. Is there a significant local and global deviant response in each patient group?
2) In general, the interpretation of the results seems to rely on significant results for some contrasts but on others being non-significant. Why do you not look for an interaction?
3) The pattern of results across groups (Panel E; see specific comments from Rev2 and Rev3 below) was somewhat counterintuitive and raises questions about what this neural signature can tell us about the state of consciousness.
4) We found the Discussion section to be too sparse. We encourage the authors to add a discussion of the implications of these data to our understanding of the consciousness state of MCS and UWS patients.
Please also see further comments in the individual reviews.
Reviewer #1 (Recommendations for the authors):
I really enjoyed reading this paper and have comments really to clarify the experimental design and results.
The design looks like it is a 2x2 design where there is a standard or deviant that is modulated globally or locally. I think it is more complicated than that and I am happy to be wrong on this. The reason for mentioning it is that the analysis focuses on the main effects of global and local and not on the interaction between them. This seems important as the main result here is a significant effect for global and a non significant effect for local. It would be great if this could be shown as a significant interaction. If the design can is not a 2x2 maybe the authors could explain this in the manuscript to help those like me who conceptually struggled with the design.
The long term goal as described is to be able to use EEG as a diagnostic tool for post-comatose patients. It would be really helpful for the more general reader to have a clearer understanding of where this study fits in this translational pipeline.
Reviewer #2 (Recommendations for the authors):
Methodology:
1) ECG signals were determined using ICA on scalp EEG rather than actual electrodes on the chest? I suggest including some discussion on the limitations with this approach – how accurate is this approach relatively to ECG?
2) It appears that the addition and removal of peaks was performed manually? If so, there is room for subjectivity with this approach making it hard to replicate/reproduce. Can detailed information about which trials etc were excluded be provided together with the dataset, such that these results can be reproduced in the future?
3) The controls sample (N=11) is relatively quite small when compared to N=59 UWS and N=58 MCS.
Results:
4) Figure 1E – could the effect observed driven by the 4 MCS participants that appear to be outliers? I think this is important to check particularly as it seems that UWS is more similar to EMCS and the Healthy group than EMCS, which is counterintuitive – is that really the case? If so, why would that be?
5) Related to the point above, it would be helpful to know how the variance of HER looks for the other 2 groups (EMCS and Healthy). Is there a relationship between HER variance and consciousness? If not, how to interpret this result?
Discussion:
6) I was confused about the issues of specificity of HER differences vs straightforward prediction error differences in auditory evoked responses locked to the 5th sound. The results state the following: "Group-wise HER average differs from EEG activity locked to the 5th sound, as compared in the same cluster or the best cluster (MANOVA test, χ 2 153=16.6366, df=3, value=0.0008)". This seems to reflect the data displayed in Figure 1D third row? (if so, an asterisk could be placed to clearly indicate differences group differences). However, this is not well discussed. It is said: "Various tests showed that locking EEG to heartbeats is necessary to find distinctions between patients, revealing the existence of a possible auditory-cardiac synchrony 207 (Pérez et al., 2021; Pfeiffer and Lucia, 2017). This study gives evidence that HERs detect auditory conscious perception, in addition to residual signs of consciousness in resting state 209 (Candia-Rivera et al., 2021a)." I agree that this study shows that locking EEG to heartbeats shows a difference between UWC and MCS, but it doesn't seem to show that it is necessary given the statistical difference reported for EEG locked to the 5th sound (best cluster). This should be clarified and discussed. What are the implications if it's not specific?
7) Links are made to studies on social cognition and the global workspace theory but I couldn't see how these data really speak to those theories. The abstract clearly states how this work could be useful in informing diagnosis of the state of consciousness, which is in keeping with the data, and yet the discussion glosses over that.
8) How do the authors interpret the fact that the HER effect is present for global but nor for local deviants?
Reviewer #3 (Recommendations for the authors):
I found the Discussion section to be too sparse, especially for a general Neuro journal like eLife. I encourage the authors to add a discussion of the implications of these data to our understanding of the consciousness state of MCS and UWS patients. Similarly, the intro should have motivated the specific paradigm used here (local-global) in more detail. Why is this a particularly useful stimulus?
From an applied perspective – Effects were perhaps present at the group level but the patients show so much variability (more than the two control groups..)….what is the vision for using an approach like this to diagnose consciousness?
[Editors' note: further revisions were suggested prior to acceptance, as described below.]
Thank you for resubmitting your work entitled "Conscious processing of global and local auditory irregularities causes differentiated heartbeat-evoked responses" for further consideration by eLife. Your revised article has been evaluated by Andrew King (Senior Editor) and a Reviewing Editor.
The manuscript has been improved but there are key remaining issues that need to be addressed, as outlined below:
1) The post-hoc decision to remove the control data is worrying, especially since the data we originally saw raised some concerns that undermined the main conclusions in the manuscript. The justification for setting the exclusion criteria as they were is not very clear, and instead, it is preferable for the control group data to be improved (e.g. by acquiring appropriate data) and re-included.
2) Additionally, it is difficult to evaluate the nature of any effects since no scalp level (time domain) data are being presented.
3) Please also see comments from Reviewer 2 below regarding clarification and interpretation.
Reviewer #2 (Recommendations for the authors):
This paper investigates the ERPs and HERs evoked in a global/local MMN paradigm in MCS and UWS patients. The critical claim is that local and global effects produce distinct ERPs and HERs for the two groups of patients, which can help distinguish between them and hence improve diagnosis.
It would be really important to understand how much HERs improve diagnosis above and beyond ERPs. If so, this would be potentially very impactful in clinical practice. By eye-balling 2B, 3B, and 4A, it seems that it might be the case but we'd need some quantification for how much more that is to be fully convinced.
I thought that the description of the results lacked some context and interpretation. More specifically, I was hoping to see more of "in order to test hypothesis X we performed the following analysis… We found Y which means Z". This applies to all results figures.
In Figures 2B and 3B, it's unclear what exactly is meant by "the clustered effects were combined into a single value" – can the authors clarify what the computation is? Averaged across time points, or something else?
"The local effect, as evaluated with HERs, showed a better separability between MCS and UWS patients, and a greater specificity with respect to surrogate heartbeat analysis." Unclear what is the data/figure/analysis that supports this claim – table 2, Figure 4D? Suggest making this explicit either in the discussion or results.
"Nevertheless, the measured responses in ERPs and HERs do not separate MCS and UWS patients' groups completely – do we have a quantification of the degree of overlap?" Figure 4 is illustrative but it would be good to have some sort of quantification.
Reviewer #3 (Recommendations for the authors):
This revised manuscript differs substantially from the originally submitted manuscript. A Post Hoc inclusion criterion imposed on the data resulted in the removal of the control group altogether. I do not think this is correct to do. That group was important to allow one to compare responses in patients relative to controls. The appropriate course of action, if it is deemed that original data were not of sufficient quality is to collect more data.
This, and the fact that ERP responses are not plotted (e.g. in Figure 2, 3) make it very difficult to interpret findings.
I am not an expert in heart-brain interactions (but am an expert in EEG/auditory oddball responses) and found it very difficult to evaluate the results without seeing the actual EEG time-domain data.
https://doi.org/10.7554/eLife.75352.sa1Author response
Essential revisions:
We found the work potentially very interesting, however several key issues, critical for supporting the claims in this paper, were identified. We hope you can address these in a revision.
1) We were confused by the specificity of HER differences vs straightforward prediction error differences in auditory evoked responses. Is there a significant local and global deviant response in each patient group?
2) In general, the interpretation of the results seems to rely on significant results for some contrasts but on others being non-significant. Why do you not look for an interaction?
3) The pattern of results across groups (Panel E; see specific comments from Rev2 and Rev3 below) was somewhat counterintuitive and raises questions about what this neural signature can tell us about the state of consciousness.
4) We found the Discussion section to be too sparse. We encourage the authors to add a discussion of the implications of these data to our understanding of the consciousness state of MCS and UWS patients.
Please also see further comments in the individual reviews.
Since one of the main concerns from reviewers and the editor was that healthy participants did not show an effect to the global effect, we realized that the previous analysis included participants where only a very limited amount of data was obtained. We now (properly) apply an inclusion criteria specifying that participants’ data should include at least 4 blocks (2 XX and 2 XY; Figure 1). With this new criterion, the new sets are 46 MCS and 40 UWS. The specific response to editor’s points, as follows:
(1) Based on our new results. Yes, there is a differentiated response to local and global effects, in both ERPs and HERs. MCS patients present repeatedly a larger response in all the comparisons.
(2) We have performed a simple correlation analysis to show that there is a distinction with respect to local and global deviants.
(3) The absence of correlates of consciousness in healthy participants (and EMCS) was due to the inclusion of participants’ data which were way too small to be reliable. Therefore, the new inclusion criteria did not include any EMCS or healthy participants.
(4) We have included a more comprehensive discussion in this revision, including the most recent findings on brain-heart interactions and conscious processing of exteroceptive information.
Reviewer #1 (Recommendations for the authors):
I really enjoyed reading this paper and have comments really to clarify the experimental design and results.
The design looks like it is a 2x2 design where there is a standard or deviant that is modulated globally or locally. I think it is more complicated than that and I am happy to be wrong on this. The reason for mentioning it is that the analysis focuses on the main effects of global and local and not on the interaction between them. This seems important as the main result here is a significant effect for global and a non significant effect for local. It would be great if this could be shown as a significant interaction. If the design can is not a 2x2 maybe the authors could explain this in the manuscript to help those like me who conceptually struggled with the design.
We thank the reviewer for pointing to the data analysis description, which may allow future readers for a better understanding of the study design.
The comparisons done are between MCS and UWS patients for the following conditions:
Auditory evoked potential related to the local effect (contrast of local deviant versus local standard EEG activity locked to the auditory stimuli)
Auditory evoked potential related to the global effect (contrast of global deviant versus local standard EEG activity locked to the auditory stimuli)
Heartbeat evoked potential related to the local effect (contrast of local deviant versus local standard EEG activity locked to the heart R-peak)
Heartbeat evoked potential related to the global effect (contrast of global deviant versus local standard EEG activity locked to the heart R-peak)
We have modified the Materials and methods to clarify on that:
“Data analysis
Two neural signatures were computed to compare MCS and UWS patients: ERPs, that relate to the average of EEG epochs locked to the auditory stimuli, and HERs that relate to the average of EEG epochs locked to the heartbeats that follow the auditory stimuli. The experimental conditions, in which ERPs and HERs were used to compare MCS and UWS patients, are:
Local effect: average of the EEG epoch associated to local deviants (local deviant/global standard epochs + local deviant/global deviant epochs), minus the average of EEG epochs associated to local standards (local standard/global standard epochs + local standard/global deviant epochs).
Global effect: average of the EEG epoch associated to global deviants (local standard/global deviant epochs + local deviant/global deviant epochs), minus the average of EEG epochs associated to global standards (local standard/global standard epochs + local deviant/global standard epochs).
Additionally, HERs average and HERs variance were analyzed during the whole experimental protocol, i.e., the neural responses to heartbeats were analyzed with respect all heartbeats independently of stimuli.”
We have split those results in two new figures (2 and 3) to clarify on the differences between local and global effects.
The long term goal as described is to be able to use EEG as a diagnostic tool for post-comatose patients. It would be really helpful for the more general reader to have a clearer understanding of where this study fits in this translational pipeline.
We have included in the discussion a paragraph explaining the potential contribution of our work in the clinical practice:
“A plethora of complementary neuroimaging techniques have been proposed to enhance the consciousness diagnosis, including anatomical and functional magnetic resonance imaging and positron emission tomography (Kondziella et al., 2020; Sanz et al., 2021). However, those methodologies may not be accessible in all clinical setups, because of costs or medical contraindications. The foregoing evidence of EEG-based techniques to diagnose consciousness (Bai et al., 2021; Engemann et al., 2018) shows promising and low-cost opportunities to develop diagnostic methods that can capture residual consciousness. Our results contribute more evidence of the potential of EEG as a diagnostic tool, but also to the role of visceral signals in consciousness (Azzalini et al., 2019; Candia-Rivera, 2022; Sattin et al., 2020). This study gives evidence that HERs detect auditory conscious perception, in addition to the residual signs of consciousness in resting-state (Candia-Rivera et al., 2021a).”
Reviewer #2 (Recommendations for the authors):
Methodology:
1) ECG signals were determined using ICA on scalp EEG rather than actual electrodes on the chest? I suggest including some discussion on the limitations with this approach – how accurate is this approach relatively to ECG?
We have included a new paragraph in Materials and methods section to clarify on the reliability of using ICA-ECG when the ECG is not available: “From this, ICA-corrected EEG data and an electrocardiogram derived from independent component analysis (ICA-ECG) is obtained. Note that the use of ICA-ECG instead of a standard ECG measured from the rib cage was successfully used in other two studies (Candia-Rivera et al., 2021a; Raimondo et al., 2017). Furthermore, it was shown that the differences between the R-peak timings obtained from the ECG and ICA-ECG differ in a range of 0-4 ms (Candia-Rivera et al., 2021a).”
2) It appears that the addition and removal of peaks was performed manually? If so, there is room for subjectivity with this approach making it hard to replicate/reproduce. Can detailed information about which trials etc were excluded be provided together with the dataset, such that these results can be reproduced in the future?
The methodology does not rely on the user capacity to identify R-peaks. The procedure of R-peak detection is performed by an automatic R-peak template matching method, which is reliable and tested in several other studies.
The detection of ectopic interbeat intervals was performed automatically as well, by detecting peaks on the derivative of the heart rate. As a final step, a visual overview of the automatically detected ectopic intervals is performed for manual corrections.
We have modified the Materials and methods section to clarify on this point:
“Heartbeats were detected on the ICA-ECG using an automated process based on a sliding time window detecting local maxima (R-peaks). Both peak detection and resulting histogram of interbeat interval duration were visually inspected in each patient. Ectopic interbeat intervals were automatically identified for review by detecting peaks on the derivative of the interbeat intervals time series. Manual addition/removal of peaks was performed if needed (23 ± 3 SEM manual corrections to individual heartbeats on average).”
3) The controls sample (N=11) is relatively quite small when compared to N=59 UWS and N=58 MCS.
The new inclusion criteria did not include any of the 11 controls because of not enough trials available for those participants.
Results:
4) Figure 1E – could the effect observed driven by the 4 MCS participants that appear to be outliers? I think this is important to check particularly as it seems that UWS is more similar to EMCS and the Healthy group than EMCS, which is counterintuitive – is that really the case? If so, why would that be?
Since this revision included a different group of patients. we have performed the analyses again, including a figure showing the distribution of the clustered effects found, to show there is a clear group trend in MCS patients to present overall larger responses (ERPs and HERs).However, outliers are expected in patients with disorders of consciousness. We have included a paragraph in the discussion about this:
“Note that outliers are expected in disorders of consciousness and exact physiological characterization of the different levels of consciousness remains challenging. First, the standard assessment of consciousness based on behavioral measures has shown a high rate of misdiagnosis in MCS and UWS (Stender et al., 2014). The cause of the misdiagnosis of consciousness arises because consciousness does not necessarily translate into overt behavior (Hermann et al., 2021). Unresponsive and minimally conscious patients, namely non-behavioral MCS (Thibaut et al., 2021), represent the main diagnostic challenge in clinical practice. Second, some of these patients suffer from conditions that may translate to no response to stimuli, even in presence of consciousness. For instance, when they suffer from constant pain, fluctuations in arousal levels, or sensory impairments caused by brain damage (Chennu et al., 2013). Third, these patients were recorded in clinical setups, which may lead to a lower signal-to-noise ratio, and lead to biased measurements in evoked potentials (Clayson et al., 2013).”
5) Related to the point above, it would be helpful to know how the variance of HER looks for the other 2 groups (EMCS and Healthy). Is there a relationship between HER variance and consciousness? If not, how to interpret this result?
It was shown in Candia-Rivera et al., 2021 (J Neurosci) in an independent cohort of UWS and MCS patients that HER variance in the right hemisphere contributed to the classification of these patients up to 87% accuracy. Importantly, HER variance in that specific scalp region do not separate by itself patients’ groups, and it rather contribute to all features used in the automatic classifier (HER average and variance in all channels at different timings between 200-400 ms). In this study we show that HER variance also may contribute to distinguish UWS and MCS patients. Likewise, that measure cannot fully separate these patients’ groups in this cohort.
Note that HER variance is a measure not explored before Candia-Rivera et al., 2021. Therefore, no further evidence exists on this marker in healthy participants, nor other paradigms. Given the sample size limitation of these groups in the initial inclusion criteria: EMCS (n=20) and healthy (n=10), and the new inclusion criteria did not include EMCS and healthy participants, we did not explore further differences on HER variance on those participants.
Discussion:
6) I was confused about the issues of specificity of HER differences vs straightforward prediction error differences in auditory evoked responses locked to the 5th sound. The results state the following: "Group-wise HER average differs from EEG activity locked to the 5th sound, as compared in the same cluster or the best cluster (MANOVA test, χ 2 153=16.6366, df=3, value=0.0008)". This seems to reflect the data displayed in Figure 1D third row? (if so, an asterisk could be placed to clearly indicate differences group differences). However, this is not well discussed. It is said: "Various tests showed that locking EEG to heartbeats is necessary to find distinctions between patients, revealing the existence of a possible auditory-cardiac synchrony 207 (Pérez et al., 2021; Pfeiffer and Lucia, 2017). This study gives evidence that HERs detect auditory conscious perception, in addition to residual signs of consciousness in resting state 209 (Candia-Rivera et al., 2021a)." I agree that this study shows that locking EEG to heartbeats shows a difference between UWC and MCS, but it doesn't seem to show that it is necessary given the statistical difference reported for EEG locked to the 5th sound (best cluster). This should be clarified and discussed. What are the implications if it's not specific?
We thank the reviewer for pointing to the interpretation of the results and statistics.
We have re-run all analyses and we have kept only a correlation analysis to show that the different markers may likely represent different cognitive processes that contribute to the consciousness assessment.
7) Links are made to studies on social cognition and the global workspace theory but I couldn't see how these data really speak to those theories. The abstract clearly states how this work could be useful in informing diagnosis of the state of consciousness, which is in keeping with the data, and yet the discussion glosses over that.
We have included in the introduction the motivation of applying the local-global paradigm:
“We hypothesized that HERs can be modulated by contextual processing of different levels of auditory regularities, as presented in the local-global paradigm (Bekinschtein et al., 2009). In this study, we analyze HERs following the presentation of auditory irregularities, with special regard on distinguishing UWS (n=40) and MCS (n=46) patients. Note that the automated classification of this cohort was previously performed in another study (Raimondo et al., 2017). Therefore, our aim is to characterize the group-wise differences between UWS and MCS patients that may allow a multi-dimensional cognitive evaluation to infer the presence of consciousness (Sergent et al., 2017), but also complement the bedside diagnosis performed with neuroimaging methods that capture neural correlates of covert consciousness (Sanz et al., 2021).”
8) How do the authors interpret the fact that the HER effect is present for global but nor for local deviants?
Indeed, with the new analyses we now show that both, local and global responses exist. We have added in the discussion the interpretation of the results:
“We showed that ERPs and HERs are repeatedly larger in MCS patients, as compared to UWS, in both local and global effects. Furthermore, the ERPs and HERs (both for the local and global effects) are uncorrelated in all possible comparisons (see Figure 4A), in addition to the results showing differentiation of clustering effects in HER and ERP (see Figure 4B). These results suggest that the neuronal mechanisms behind these ERPs and HERs responses are independent. In addition, we found that HER variance is higher in MCS patients than in UWS patients, as previously reported in resting state (Candia-Rivera et al., 2021a). Put together these results suggest that two different neuronal signatures differentiate MCS from UWS patients. A first process probed with HER variability differentiates, irrespective of the current stimulus type being processed. This first process originates from central and right temporal scalp areas and has been linked with social cognition but could also correspond to a self-consciousness-state marker (Candia-Rivera et al., 2021a). Second, a modulation of HER in response to local and global auditory irregularities. These responses present several properties related to a neural signature of conscious access to local and global deviant stimuli. Such ERPs and HERs modulations by conscious access to a new stimulus attribute may well correspond to a self-consciousness updating process occurring ‘downstream’ to conscious access (Sergent and Naccache, 2012), and enabled for instance in a global neuronal workspace architecture (Dehaene and Naccache, 2001).”
Reviewer #3 (Recommendations for the authors):
I found the Discussion section to be too sparse, especially for a general Neuro journal like eLife. I encourage the authors to add a discussion of the implications of these data to our understanding of the consciousness state of MCS and UWS patients. Similarly, the intro should have motivated the specific paradigm used here (local-global) in more detail. Why is this a particularly useful stimulus?
From an applied perspective – Effects were perhaps present at the group level but the patients show so much variability (more than the two control groups..)….what is the vision for using an approach like this to diagnose consciousness?
Thanks for this recommendation. We have enriched the discussion in this new revision.
We have included a commentary on the potential of the local-global paradigm:
“We showed that ERPs and HERs are repeatedly larger in MCS patients, as compared to UWS, in both local and global effects. Furthermore, the ERPs and HERs (both for the local and global effects) are uncorrelated in all possible comparisons (see Figure 4A), in addition to the results showing differentiation of clustering effects in HER and ERP (see Figure 4B). These results suggest that the neuronal mechanisms behind these ERPs and HERs responses are independent. In addition, we found that HER variance is higher in MCS patients than in UWS patients, as previously reported in resting state (Candia-Rivera et al., 2021a). Put together these results suggest that two different neuronal signatures differentiate MCS from UWS patients. A first process probed with HER variability differentiates, irrespective of the current stimulus type being processed. This first process originates from central and right temporal scalp areas and has been linked with social cognition but could also correspond to a self-consciousness-state marker (Candia-Rivera et al., 2021a). Second, a modulation of HER in response to local and global auditory irregularities. These responses present several properties related to a neural signature of conscious access to local and global deviant stimuli. Such ERPs and HERs modulations by conscious access to a new stimulus attribute may well correspond to a self-consciousness updating process occurring ‘downstream’ to conscious access (Sergent and Naccache, 2012), and enabled for instance in a global neuronal workspace architecture (Dehaene and Naccache, 2001).”
We have included a commentary on where our results stand within the brain-heart interaction literature:
“Our results contribute to the extensive experimental evidence showing that brain-heart interactions, as measured with HERs, are related to perceptual awareness (Azzalini et al., 2019; Skora et al., 2022). For instance, neural responses to heartbeats correlate with perception in a visual detection task (Park et al., 2014). Further evidence exists on somatosensory perception, where a higher detection of somatosensory stimuli occurs when the cardiac cycle is in diastole and it is reflected in HERs (Al et al., 2020). Evidence on heart transplanted patients shows that the ability of heartbeats sensation is reduced after surgery and recovered after one year, with the evolution of the heartbeats sensation recovery reflected in the neural responses to heartbeats as well (Salamone et al., 2020). The responses to heartbeats also covary with self-perception: bodily-self-identification of the full body (Park et al., 2016), and face (Sel et al., 2017), and the self-relatedness of spontaneous thoughts (Babo-Rebelo et al., 2016) and imagination (Babo-Rebelo et al., 2019). Moreover, brain-heart interactions measured from heart rate variability correlate with conscious auditory perception as well (Banellis and Cruse, 2020; Pérez et al., 2021; Pfeiffer and Lucia, 2017).”
We have included a commentary on the clinical impact of our findings:
“A plethora of complementary neuroimaging techniques have been proposed to enhance the consciousness diagnosis, including anatomical and functional magnetic resonance imaging and positron emission tomography (Kondziella et al., 2020; Sanz et al., 2021). However, those methodologies may not be accessible in all clinical setups, because of costs or medical contraindications. The foregoing evidence of EEG-based techniques to diagnose consciousness (Bai et al., 2021; Engemann et al., 2018) shows promising and low-cost opportunities to develop diagnostic methods that can capture residual consciousness. Our results contribute more evidence of the potential of EEG as a diagnostic tool, but also to the role of visceral signals in consciousness (Azzalini et al., 2019; Candia-Rivera, 2022; Sattin et al., 2020). This study gives evidence that HERs detect auditory conscious perception, in addition to the residual signs of consciousness in resting-state (Candia-Rivera et al., 2021a).”
[Editors' note: further revisions were suggested prior to acceptance, as described below.]
The manuscript has been improved but there are key remaining issues that need to be addressed, as outlined below:
1) The post-hoc decision to remove the control data is worrying, especially since the data we originally saw raised some concerns that undermined the main conclusions in the manuscript. The justification for setting the exclusion criteria as they were is not very clear, and instead, it is preferable for the control group data to be improved (e.g. by acquiring appropriate data) and re-included.
2) Additionally, it is difficult to evaluate the nature of any effects since no scalp level (time domain) data are being presented.
3) Please also see comments from Reviewer 2 below regarding clarification and interpretation.
We appreciate the editor's comments and acknowledge that it would be ideal validating our results with a larger cohort. In the first revision, we recognized that the unrestricted inclusion criteria inadvertently compromised the statistical power of our study. Consequently, the results did not align with our expectations, particularly in relation to the healthy controls. This heterogeneity within the statistical analysis potentially led to an overestimation of the observed effects.
To address these issues, we decided to narrow our focus in the second version of this manuscript. We specifically targeted the population of interest, allowing us to investigate the underlying factors that differentiate MCS and UWS/VS patients. By refining the inclusion criteria, we were able to establish a clearer contrast between the two patients’ groups. This refinement facilitated a more accurate assessment of the impact of auditory irregularities on the measures of brain-heart interaction that were studied.
We understand the concerns raised about the exclusion of the healthy control group. In this revision, we have re-included them, but solely for qualitative analysis purposes. Our intention was to address the limitation of the current population by demonstrating that the new results obtained from comparing MCS and UWS/VS patients exhibit more reliable differences, as MCS generally align with the expected trends observed in healthy controls.
We fully acknowledge the potential concerns raised regarding the exclusion and subsequent re-inclusion of the healthy control group. In order to justify this decision, we would like to provide a detailed explanation of how it strengthens the robustness and validity of our findings.
Furthermore, we would like to stress that due to current circumstances, acquiring new data has become very challenging, particularly because some of the authors are no longer affiliated with the laboratory where this study was conducted.
Considering these justifications, we kindly request that you consider our rationale for including healthy controls in the study analysis during the second revision of our manuscripts. We have prepared a revised version of the manuscript that incorporates the initial 11 healthy controls for qualitative analysis. We kindly request the editor and reviewers to evaluate our revised proposal, which we believe adequately addresses your concerns regarding our results. We believe that this decision significantly contributes to the methodological soundness and validity of our research.
Thank you for your time and consideration. We appreciated your valuable insights and feedback, which undoubtedly contributed to improving the quality of our study. Please find our responses to the specific comments from the reviewers below. The first and second points are further addressed in our responses to reviewer 3.
Reviewer #2 (Recommendations for the authors):
This paper investigates the ERPs and HERs evoked in a global/local MMN paradigm in MCS and UWS patients. The critical claim is that local and global effects produce distinct ERPs and HERs for the two groups of patients, which can help distinguish between them and hence improve diagnosis.
It would be really important to understand how much HERs improve diagnosis above and beyond ERPs. If so, this would be potentially very impactful in clinical practice. By eye-balling 2B, 3B, and 4A, it seems that it might be the case but we'd need some quantification for how much more that is to be fully convinced.
We thank the reviewer for their comments. We have included a panel C in Figure 4 a new analysis performing a linear discriminant classifier to quantify the complementarity of the ERPs and HERs
I thought that the description of the results lacked some context and interpretation. More specifically, I was hoping to see more of "in order to test hypothesis X we performed the following analysis… We found Y which means Z". This applies to all results figures.
We have included a short paragraph to explicitly state the objective of the study:
“In this study, we examined the cognitive processing of auditory irregularities in patients with disorders of consciousness using the local-global paradigm. This paradigm assesses the processing of both local (short-term) and global (long-term) auditory regularities. Our objective was to identify physiological responses that could differentiate between patients in MCS and those in UWS. We hypothesized that assessing auditory irregularities at both local and global levels could offer valuable insights into the distinction of MCS and UWS patients. Furthermore, this distinction may be further improved by analyzing the physiological modulation of auditory processing in relation to measures of brain-heart interactions. To achieve this, we conducted tests to investigate the local and global effects in ERPs, which involved analyzing the standard average of EEG epochs aligned with the occurrence of auditory deviants. Additionally, we explored the HERs to assess whether the neural responses to heartbeats, within the context of auditory irregularity processing, could serve as novel differentiating factors between MCS and UWS patients.”
In Figures 2B and 3B, it's unclear what exactly is meant by "the clustered effects were combined into a single value" – can the authors clarify what the computation is? Averaged across time points, or something else?
We thank the reviewer for this comment. We have included a description of the averaging procedure, as follows:
“The clustered effects were combined to obtain a single value for each patient, corresponding to ERP global and local effects. To combine the clustered effects, we computed the average of all points (channel x time) identified in the cluster permutation analysis, which effectively distinguished between patients diagnosed with MCS and UWS.”
"The local effect, as evaluated with HERs, showed a better separability between MCS and UWS patients, and a greater specificity with respect to surrogate heartbeat analysis." Unclear what is the data/figure/analysis that supports this claim – table 2, Figure 4D? Suggest making this explicit either in the discussion or results.
We thank the reviewer for this comment. We have included a description of that result, as follows:
“It is worth noting that the HER local effect demonstrated higher specificity compared to the HER global effect during the permutation test. Only 3% of randomly timed surrogate heartbeats exhibited separability that surpassed what was observed with the original heartbeats.”
"Nevertheless, the measured responses in ERPs and HERs do not separate MCS and UWS patients' groups completely – do we have a quantification of the degree of overlap?" Figure 4 is illustrative but it would be good to have some sort of quantification.
We thank the reviewer for this comment. As mentioned above, we included a new analysis on patients’ classification. The overlap in classifications is shown in the confusion matrices in Figure 4C.
Reviewer #4 (Recommendations for the authors):
This revised manuscript differs substantially from the originally submitted manuscript. A Post Hoc inclusion criterion imposed on the data resulted in the removal of the control group altogether. I do not think this is correct to do. That group was important to allow one to compare responses in patients relative to controls. The appropriate course of action, if it is deemed that original data were not of sufficient quality is to collect more data.
We appreciate the reviewer's comment. We have made a few modifications to answer to the reviewer’s concerns.
In the new figures, we have incorporated the initial 11 healthy controls as a reference group. Although the healthy controls had fewer trials compared to the patients, we included them to provide context based on the new inclusion criteria. We have clarified this in the participants description as follows:
“The healthy controls participating in this study completed two blocks of the local-global paradigm, one XX and one XY. It is important to note that they were included solely as a reference group for qualitative analyses. The purpose of including healthy controls in our study was to determine if MCS patients exhibit similar trends in markers where a differentiation between MCS and UWS/VS patients was observed.”
In the previous version of the manuscript, the healthy controls did not exhibit the expected trend in the measured HERs. However, with the analysis conducted using the new inclusion criteria, we observed different clustered effects between the comparisons of MCS and UWS, which also affected the trend observed in the healthy controls. In this revised version of the manuscript, we have included again the distributions of the healthy controls as a reference point.
Our findings demonstrate that healthy controls exhibit a similar trend to MCS patients in ERP local, HER global, and HER local. However, the ERP global effect was the only feature that deviated from this trend, as discussed below:
“Furthermore, it is worth noting that the ERP global effect observed in healthy controls did not follow the same trend than MCS patients. These findings may require of further future explorations to determine if the observed effect is exclusive to MCS patients or if healthy controls do not exhibit the same effect due to their lower number of trials performed in the local-global paradigm during this study. However, the response observed in healthy controls does resemble a standard P300 response. These findings align with previous reports indicating that the ERPs during local deviants exhibit superior discriminatory ability between MCS and UWS patients (Faugeras et al., 2012). Furthermore, these results suggest that both ERP and HER in processing local auditory irregularities might be predominant for distinguishing between MCS and UWS. This notion is further supported by the higher accuracy of the linear discriminant classifier in classifying MCS and UWS patients by using ERP local and both HER global and local effects, as compared to all other possible feature combinations. Nonetheless, the inclusion of global effects marginally improved the classification performance, indicating that although the global effects are weaker than the local effects, they might provide complementary information to the local effects.”
This, and the fact that ERP responses are not plotted (e.g. in Figure 2, 3) make it very difficult to interpret findings.
I am not an expert in heart-brain interactions (but am an expert in EEG/auditory oddball responses) and found it very difficult to evaluate the results without seeing the actual EEG time-domain data.
We thank the reviewer for this comment. As shown above, we have included a new panel C in the figures 2 and 3 with the time-varying responses for ERPs and HERs.
https://doi.org/10.7554/eLife.75352.sa2Article and author information
Author details
Diego Candia-Rivera

Catherine Tallon-Baudry
Funding
Canadian Institute for Advanced Research
- Catherine Tallon-Baudry
Agence Nationale de la Recherche (ANR-17-EURE-0017)
- Catherine Tallon-Baudry
Agence Nationale de la Recherche (ANR-10- IAIHU-06)
- Jacobo D Sitt
Sorbonne Université (EMERGENCE)
- Jacobo D Sitt
European Commission (JTC2019)
- Jacobo D Sitt
The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication.
Acknowledgements
We thank all of the participants who took part in the studies. We would like to thank the work and support of the clinicians at the Neuro ICU, DMU Neurosciences, APHP- Sorbonne Université, Hôpital de la Pitié Salpêtrière, Paris, France; and the patient families whose consent and understanding are essential to the progress of the field.
Ethics
The study was approved by the ethics committee of CPP Île de France 1 (Paris, France). Informed consent was signed by the patients' legal representatives for approval of participation in the study, as required by the declaration of Helsinki. (NEURO-DoC/HAO-84 006/20130409 and M-NEURO-DoC/NCT04534777).
Senior and Reviewing Editor
- Andrew J King, University of Oxford, United Kingdom
Reviewers
- Marta Garrido
- Maria Chait, University College London, United Kingdom
Version history
- Preprint posted: October 28, 2021 (view preprint)
- Received: November 7, 2021
- Accepted: October 24, 2023
- Accepted Manuscript published: October 27, 2023 (version 1)
- Version of Record published: November 15, 2023 (version 2)
Copyright
© 2023, Candia-Rivera et al.
This article is distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use and redistribution provided that the original author and source are credited.
Metrics
-
- 479
- Page views
-
- 97
- Downloads
-
- 1
- Citations
Article citation count generated by polling the highest count across the following sources: PubMed Central, Crossref, Scopus.
Download links
A two-part list of links to download the article, or parts of the article, in various formats.
Downloads (link to download the article as PDF)
Open citations (links to open the citations from this article in various online reference manager services)
Cite this article (links to download the citations from this article in formats compatible with various reference manager tools)
Conscious processing of global and local auditory irregularities causes differentiated heartbeat-evoked responses
eLife 12:e75352.
https://doi.org/10.7554/eLife.75352
Further reading
-
- Neuroscience
Postsynaptic mitochondria are critical for the development, plasticity, and maintenance of synaptic inputs. However, their relationship to synaptic structure and functional activity is unknown. We examined a correlative dataset from ferret visual cortex with in vivo two-photon calcium imaging of dendritic spines during visual stimulation and electron microscopy reconstructions of spine ultrastructure, investigating mitochondrial abundance near functionally and structurally characterized spines. Surprisingly, we found no correlation to structural measures of synaptic strength. Instead, we found that mitochondria are positioned near spines with orientation preferences that are dissimilar to the somatic preference. Additionally, we found that mitochondria are positioned near groups of spines with heterogeneous orientation preferences. For a subset of spines with a mitochondrion in the head or neck, synapses were larger and exhibited greater selectivity to visual stimuli than those without a mitochondrion. Our data suggest mitochondria are not necessarily positioned to support the energy needs of strong spines, but rather support the structurally and functionally diverse inputs innervating the basal dendrites of cortical neurons.
-
- Neuroscience
Several discrete groups of feeding-regulated neurons in the nucleus of the solitary tract (nucleus tractus solitarius; NTS) suppress food intake, including avoidance-promoting neurons that express Cck (NTSCck cells) and distinct Lepr- and Calcr-expressing neurons (NTSLepr and NTSCalcr cells, respectively) that suppress food intake without promoting avoidance. To test potential synergies among these cell groups we manipulated multiple NTS cell populations simultaneously. We found that activating multiple sets of NTS neurons (e.g., NTSLepr plus NTSCalcr (NTSLC), or NTSLC plus NTSCck (NTSLCK)) suppressed feeding more robustly than activating single populations. While activating groups of cells that include NTSCck neurons promoted conditioned taste avoidance (CTA), NTSLC activation produced no CTA despite abrogating feeding. Thus, the ability to promote CTA formation represents a dominant effect but activating multiple non-aversive populations augments the suppression of food intake without provoking avoidance. Furthermore, silencing multiple NTS neuron groups augmented food intake and body weight to a greater extent than silencing single populations, consistent with the notion that each of these NTS neuron populations plays crucial and cumulative roles in the control of energy balance. We found that silencing NTSLCK neurons failed to blunt the weight-loss response to vertical sleeve gastrectomy (VSG) and that feeding activated many non-NTSLCK neurons, however, suggesting that as-yet undefined NTS cell types must make additional contributions to the restraint of feeding.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}